This is an updated version of a previously published blog post I wrote on the topic of my opposition to Fluoride being added to Calgary’s water supply. With the upcoming plebiscite on the issue scheduled for the October 2021 civic election, and the large amount of fresh research on the topic, I decided to update the blog.
Calgary successfully removed Fluoride from the water in 2011, on the basis of the need for costly plant upgrades to continue, and the rights of individuals to not be medicated against their will, as well as attention to the fact the Fluoride is not a substitute for dental care for poor children, which would be far more effective in preventing dental decay. The funding used to fluoridate water was redirected instead into a program of dental care for low income children.
The catalyst for this reconsideration seems to be a study from the University of Calgary study by Mclaren et al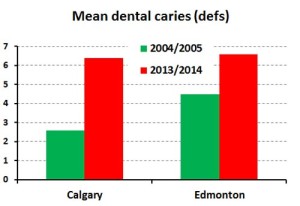 . In this study they compared the number of cavities in grade two schoolchildren between Calgary, which stopped Fluoridation, and Edmonton, which continued it. The study was done in 2013-14, and a similar study in 2004-5 was used a control. The study results are displayed in graphical form to the right:
. In this study they compared the number of cavities in grade two schoolchildren between Calgary, which stopped Fluoridation, and Edmonton, which continued it. The study was done in 2013-14, and a similar study in 2004-5 was used a control. The study results are displayed in graphical form to the right:
Now, this would seem to be quite an open and shut case. However, As recently discussed by Neurath et al in another article, this survey was however, somewhat odd in using older 2004-5 data, instead of a more recent 2009-10 survey 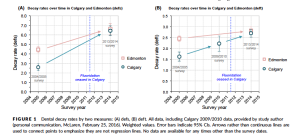 of dental health in Calgary. This 2009-10 survey was performed using the same methods, in fact being intended to be compared to the 2004-5 study, and it gives some remarkable results, as shown in the figure to the left (taken from page 3 of Neurath et al’s paper, and gratefully acknowledged).
of dental health in Calgary. This 2009-10 survey was performed using the same methods, in fact being intended to be compared to the 2004-5 study, and it gives some remarkable results, as shown in the figure to the left (taken from page 3 of Neurath et al’s paper, and gratefully acknowledged).
From Neurath’s data we can see that the vast majority of change in dental decay rates occurred before the cessation  of fluoridation in the city. The rate of dental decay between 2009-10 and 2013-14 in fact, while showing an upward trend, were not statistically significantly different. Neurath also criticized Mclaren for equating Calgary and Edmonton, as Edmonton has always had considerably poorer health than Calgary, and at baseline Edmonton’s tooth decay rate was 73% higher, for reasons that are not clear, making comparisons between the two of limited value. There was also some potential for selection bias in the 2013-14 dental survey, and subgroup analysis, restricting analysis to children with at least one cavity in fact are even less persuasive than the all inclusive data, as shown in the figure to the right, again gratefully acknowledged as being taken from Neurath et al.
of fluoridation in the city. The rate of dental decay between 2009-10 and 2013-14 in fact, while showing an upward trend, were not statistically significantly different. Neurath also criticized Mclaren for equating Calgary and Edmonton, as Edmonton has always had considerably poorer health than Calgary, and at baseline Edmonton’s tooth decay rate was 73% higher, for reasons that are not clear, making comparisons between the two of limited value. There was also some potential for selection bias in the 2013-14 dental survey, and subgroup analysis, restricting analysis to children with at least one cavity in fact are even less persuasive than the all inclusive data, as shown in the figure to the right, again gratefully acknowledged as being taken from Neurath et al.
This paper was responded to by Mclaren who stated that the 2009-10 data were excluded due to the lack of a comparison survey in Edmonton, and due to the 2010 paper’s focus on whole tooth, rather than tooth surface data, and dispute several other factors in Neurath’s analysis.
Regardless of this, it can be seen that the case for fluoridation based on this single paper in Calgary is not particularly strong. Calgary and Edmonton ( and indeed most of the first world) is in the midst of a vast increase in dental decay, likely mediated by changes in diet. Fluoridation however, like all interventions on the human body, does not exclusively affect one organ to the exclusion of others. Fluoridation has systematic effects on the human body, outside of the teeth, and these must be taken into account.
A small subset of patients have reported clinically a negative effect on their thyroids from fluoridated water. Some research has examined this phenomenon and found no particular association between TSH levels and urinary Fluoride excretion. Aside from the issues of using TSH alone instead of a full range of thyroid lab values, other research has examined this phenomenon in light of the patients iodine status. In patients with lower Iodine status, according to this research, TSH increases, indicating an adverse effect on thyroid hormone secretion. As we can see from this data from statscan, a considerable percentage of Canadians have poor iodine status, and may have thyroid function lowered by water Fluoridation, particularly in inland areas such as Calgary, which tend to have lower iodine status.
Fluoridation of water was also associated in one study with lower rates of eye cancer, and in another with lower rates of kidney stones and bladder cancer.
The most contentious issue however remains the effect of Fluoride on children’s intelligence. A number of research studies have been done suggesting a strong correlation between Dental fluorosis and lowered IQ in Children. (see here, for a study on this topic in Bagalkot, and here for another done in Lucknow). In one metanalysis in 2012 Choi et all found an inverse association with Fluoride levels on water and children’s IQ, that is a higher levels of fluoride correlated with a lower IQ. This study has been criticized for including studies that looked at both Iodine and Fluoride status, as well as relying on naturally occurring levels of fluoride, rather than artificially supplemented by water fluoridation as well as other confounders, such as the association of water Fluoride with Arsenic contamination, and inability to determine the exact level of fluoride consumption when relying on general water concentrations. One such study, can be seen here, although it was not included in the 2012 metaanalysis. Another, grading children into high, medium and low Fluoride areas found the same negative correlation.
So, several more studies were done using much more precise measures. One in Mexico measured the urine concentration of Fluoride in pregnant women, and correlated it to their children’s cognitive test scores at age 4 and 6-12. This study found significant associations with higher Fluoride urine levels and lower performance on these cognitive tests resulting in a loss of roughly 6.13 loss in IQ for every 1mg/L increase in maternal fluoride excretion. Another study was performed using similar methods in Canada, finding a loss of 4.5 IQ points in boys for every 1mg/L, but none for girls. These last two studies overcame many of the specific problems with the 2012 metanalysis and seem to confirm the findings. To put this effect into context, high childhood lead exposure correlates with a 1.61 point loss of IQ in adulthood, and when this was found out, the result was international banning of leaded gasoline, paint and glazes. This reduction in lead in the 1970s is also hypothesized to be behind the decline in violent crime seen in the 1990s, again, with an IQ point drop that is approximately 1/3 that shown from fluoride.
Echoing the above research,and the emphasis on boys being more vulnerable to negative health outcomes from Fluoridation, another study in Mexico was performed based on urinary Fluoride excretion showing a later age of puberty in boys with higher Fluoride exposure.
More recent research has been performed examining the effect of exposure after birth, as well as confirming the effects of prenatal exposure. A Canadian study of 398 mother child pairs were analyzed for tap water fluoridation and childhood IQ. An increase of 0.5mg/ml correlated with a 9.3-6.2 point IQ drop. Even controlling for maternal exposure to fluoridated water, both breastfed infants and formula fed infants demonstrated lower IQs. A 0.5mg increase in fluoride intake in breastfed infants corresponded with an 8.8 point decrease in IQ.
Another study differentiated the effect of exposure to childhood IQ at different points in childhood development, prenatal exposure only, postnatal exposure, control, and both pre and postnatal. Mean IQ in children exposed to excessive fluoride during pregnancy was significantly lower, and they had a 51.1% decreased chance of excellent intelligence compared with children without excess exposure at any time (acknowledging of course the flawed and ethnocentric nature of IQ). For all children, urinary fluoride excretion above 1.7mg/L was negatively associated with IQ. In children without prenatal exposure, each 1mg/L increase in urinary fluoride was associated with a reduced IQ score of 11.4.
Also recently, some speculation has emerged the Fluoridation in water sources, particularly in combination with aluminum exposure in utero may predispose individuals to develop autism. The evidence behind this hypothesis has not yet been thoroughly examined however.
Conclusions:
The above data do present a complex picture. The general literature, and I personally, accepts that increasing the level of Fluoride in water decreases dental cavities. However, Fluoride also has a complex and negative effect on Childhood intelligence, likely lowering the IQ of children of mothers exposed to high fluoride exposure by 4-6 points per extra mg/L of maternal fluoride excretion. As well, post pregnancy exposure does also seem to reduce IQ. A 0.5mg increase in fluoride intake in breastfed infants corresponded with an 8.8 point decrease in IQ.
To put this into context, the mass exposure of children to leaded paint and gasoline, which was hypothesized to be behind the Lead-Crime effect, showed an approximately 1.6 point IQ drop.
As well, as we can see with more complete data, while Calgary is experiencing an increase in dental cavities in children, this is likely due to much more complex factors than just the removal of Fluoridation from the cities water supply, as the majority of the increase, and possibly all of it, occurred before Fluoride was actually removed.
Fluoride itself is also extremely difficult to remove from water, requiring complex Reverse Osmosis equipment to fully remove. Other additives to water with negative health outcomes, such as Chlorine (associated with certain types of Cancers and disruption of the gut Microbiome) are not relevant, as chlorine is easily removed by inexpensive water filters, within reach of nearly all Calgarians, and the certain benefits of removing water borne pathogens from the water supply that Chlorine provides.
The cost of Fluoridation in a city that increasingly burdened by a shrinking tax base, particularly when Fluoridation is difficult to remove from the water and will have a strong adverse effect on intelligence in children, is not in the public interest of Calgary. The problem of increased dental cavities would best be solved by public coverage of dental medicine (which should be included in an expanded medicare system along with Naturopathic, Chiropractic, Traditional Chinese, and other medicines).